Ultrasound can replace CT and MRI for neurosurgical navigation
23 Nov 2010
Aloka Holding Europe AG is working with internationally renowned neurosurgeon, Dr Klaus Resch of the University of Greifswald and Klinikum München in Germany to promote the potential for ultrasound to be used in conjunction with, or as a replacement for, CT/MRI as a neuro-navigational tool in certain operations.
As part of this initiative, Dr Resch has this month begun planning to extend his training programme for neurosurgeons across all of Latin America following a successful pilot with surgeons in Mexico [1]. He will be announcing the full results of the Latin American initiative at the Neuroendoscopy 2011 conference taking place in Guadalajara (Mexico).
Dr Resch believes ultrasound has been greatly underused in neurosurgery over the past 20 years. He said, "I strongly advise all neurosurgeons to widen their imaging tools beyond just CT and MRIs. Intra-operative ultrasound can solve many problems that cannot be achieved with other imaging techniques."
“We are discovering new surgical uses of ultrasound daily and its use in the developing world could have enormously positive implications to patient safety — as the use of CT and MRI is low in these countries due to its prohibitive costs”
Dr Resch bases his recommendation on a 1084-patient case study he conducted on the uses of ultrasound in surgery, one third of which were observed intra-operative and two thirds peri-operatively [2].
In this, he was able to prove conclusively that ultrasound was an excellent neuro-navigational system, which provided the surgeon with both real-time imaging and targeting capabilities in all of the intra-operative cases he observed (376 cases). In addition, it was also demonstrated that neurosurgical therapy outside the operating room could be markedly assisted by ultrasound.
For a number of years, Dr Resch has been a pioneer in the use of neurosurgical ultrasound and has discovered a broad variety of applications and indications both intra- and peri-operatively. He conducted his research using four bespoke Aloka probes in a variety of settings — including the TCD probe (use: intensive care unit), the small part sector probe (use: intra-operative), and the burr-hole probe (use: intra-operative).


Examples of Aloka ultrasound probes used for
neurosurgery
The findings showed that ultrasound enabled the surgeon to be more reactive during surgery, with real-time images showing exactly how the lesion is being manipulated and how the brain reacts. In plain terms, this means the surgeon can view what is happening as he operates, without the need to stop the operation to obtain new images (ie from CT or MRI), which can be very dangerous for the patient.
In addition, ultrasound is also preferable to CT or MRI during these cases as, with real-time images, there is no risk of error due to the brain shifting. Furthermore, the surgeon can also quickly locate vascular feeders and the source of any bleeding — a common and life threatening problem during operations.
|
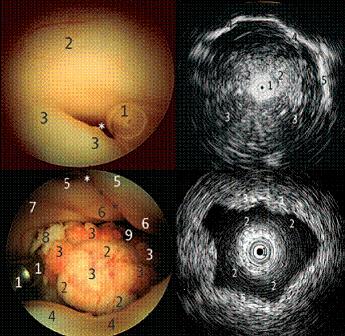
Example of ultrasound used in neurosurgery
A (top left), aqueduct. The sonoprobe (1) is entering the aqueduct (white asterisk) at the posterior third ventricle formed by hypothalamus (2) and posterior commissure (3). B (top right), aqueduct and posterior fossa. The sonoprobe (1) is inside the aqueduct of the mesencephalon (2). As the zoom is very low, the posterior fossa is scanned with the cerebellum (3), clivus, and petroclival border (4), as well as the tentorial notch on the right side (5). C (bottom left), fourth ventricle. The sonoprobe (1), as well as the inferior vermis (2) bulging into the ventricle covered by the variant of a circular plexus (3). The superior medullary velum (4) limits the inferior view while a view into the depth of the foramen of Magendi (9) is possible. The facial colliculus (6) and medial eminence (5) are seen on both sides, divided by the medial sulcus (asterisks). Laterally, the vestibular area (7) is visible, as is the entry to the foramen of Luschka (8). D (bottom right), fourth ventricle scan. The sonoprobe (1) is in the fourth ventricle looking into the parenchyma of facial colliculus (3), superior cerebellar peduncle (4), and superior medullary velum and superior vermis (5). |
Additionally, Dr Resch has shown in Mexico that ultrasound could provide an invaluable surgical tool in the developing world, where the cost of procuring an MRI or CT scanner is highly prohibitive in comparison to an ultrasound unit.
“Due to the cost-effective nature, logistical ease of use, and ergonomic character of ultrasound, it could have profound implications in the developing world and, this November, I will begin expanding my training programmes for neurosurgeons across all of Latin America. However, high-end neurosurgical ultrasound depends entirely on having selected the appropriate probes and Aloka technology has been a big contributory factor in advancing its clinical uses.”
References
1. For details of future training programmes please visit: www.ens-surgery.com
22. Resch K, Kleist-Welch Guerra W, Schroeder HWS. Use of High-end Ultrasound in Minimally Invasive Strategy of Neurosurgery: Review of 1084 Cases. Paper presented at the 13th European Congress of Neurosurgery (2007).